×
A. Your doctor should make sure you have accurate information about the abortion procedure. You should be given information on the different methods of abortion that can be used at your stage of pregnancy and the possible risks associated with them.
You should be offered extra support, including counselling if you want it, to help you make your decision. You should be offered information and support if you decide not to have an abortion.
You have the right to delay or cancel appointments. You can also change your mind about having the abortion at any stage.
You should be offered:
In some circumstances, you may be offered:
You will have an opportunity to discuss with your healthcare team your plan for contraception after the abortion.
A. An abortion is a way of ending an unwanted pregnancy using either medicines (drugs), called a medical abortion, or using a surgical procedure, called a surgical abortion.
Both types of abortion may be used at any stage of pregnancy.
If you are less than 7 weeks pregnant, a medical abortion is more likely to work than a surgical abortion.
Your abortion service should be able to offer at least one method for each stage of pregnancy. You should ideally have a choice of methods, although this may not always be possible. You will usually be able to go home the same day.
You will probably have some pain or discomfort, whatever kind of abortion you have. You should be offered a choice of appropriate pain relief if you need it.
Whichever type of abortion you have, you will be offered antibiotics to prevent infection.
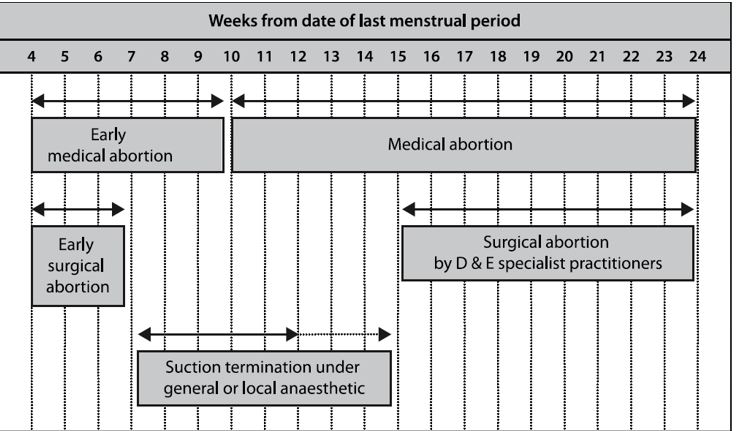
A. The various medical methods of abortion are:
Early medical abortion up to 9 weeks and 6 days of pregnancy
You will need to attend the clinic or hospital to receive two different medicines.
The first medicine you will be given is mifepristone which will block the hormones to the pregnancy. You will take the mifepristone orally whilst in clinic or hospital. The second medication misoprostol will be given to you to take home and administer yourself, if you wish to do so (48 hours after taking the first medication).
You will be given detailed instructions about when and how to use the medication by your doctor. Misoprostol is a hormone that makes your uterus (womb) expel the pregnancy, usually within 4 to 6 hours. You will be offered pain relief during the abortion. You may continue to bleed for a few days.
You should be given detailed follow up instructions about what to do if you suspect the abortion has not ended the pregnancy.
Medical abortion after 9 weeks and 6 days of pregnancy
You take the same drugs as you would for an early medical abortion.
At this stage, however, abortion takes longer and you may need to have more than one dose of prostaglandin and additional pain relief.
If you have a medical abortion between 13and 24 weeks of pregnancy, you should be cared for by an obstetrician who has appropriate experience and you will usually need to be in hospital.
A. The various surgical methods of abortion are:
Suction termination: usually from 7 to 15 weeks of pregnancy
Most doctors offer suction termination up to the 12th week of pregnancy, while some offer it up to the 15th week.
It can sometimes be used if you are less than 7 weeks pregnant.
If you have a surgical abortion, you may be offered:
The cervix (entrance to the uterus) is gently stretched and opened until it is wide enough for the contents of the uterus to be removed with a suction tube. The extent to which the cervix needs to be opened depends on the size of the pregnancy. To make this safer, there are a number of effective ways to soften the cervix beforehand, for example by inserting tablets containing misoprostol into your vagina.
Surgical dilatation and evacuation (D&E): from about 15 weeks of pregnancy
Your cervix is gently stretched and opened (this is known as dilatation) so that the pregnancy can be removed in fragments with a suction tube and forceps. An ultrasound scan should be done at the same time to reduce the risk of complications and make sure that all the pregnancy is removed. You will usually need a general anaesthetic.
A. All methods of early abortion carry a small risk of failure to end the pregnancy and therefore a need to have another procedure. This is uncommon, occurring in fewer than 1 in 100 women.
A. Abortion, at any time in pregnancy, is a safe procedure for which serious complications are uncommon. The earlier in the pregnancy you have an abortion, the safer it is. Your doctor should tell you about risks and complications that relate to the specific abortion procedure being offered to you. If you have concerns about the risks, let your doctor know so that they can tell you more.
A. Complications at the time of abortion include:
Should complications occur, treatment – including surgery – may be required.
A. You are more likely to get problems in the 2 weeks after the abortion than at the time of the procedure itself:
A. After the abortion you should be offered written information that tells you what you are likely to experience, including symptoms that you should see a doctor for urgently and symptoms of a continuing pregnancy.
A. You should start using contraception straight away. It is safe to have an intrauterine device (IUD) or intrauterine system (IUS) fitted immediately.
A. If you are RhD-negative, you should usually be offered an anti-D injection after your abortion.
A. If there were no problems with your abortion, it will not affect your future chances of becoming pregnant.
A. Abortion does not increase your risk of a miscarriage, ectopic pregnancy or a low placenta if you do have another pregnancy. However, you may have a slightly higher risk of a premature birth.
A. An abortion does not increase your risk of developing breast cancer.
A. The key points to remember are: